
ISSUES IN DIAGNOSIS: CO-MORBIDITY, CULTURE AND GENDER BIAS AND SYMPTOM OVERLAP
If you observed me sitting alone, quietly muttering to myself, you would probably conclude that I was unwell. But if you then noticed my hands were clasped, and my eyes closed, you would just as readily decide I was praying.
Should I confess to hearing voices, the diagnosis might be schizophrenia—unless I describe that voice as God. In that case, the response is likely to be one of respect, even reverence.
As Thomas Szasz observed, the difference lies not in the experience itself, but in the social interpretation placed upon it. One individual is labelled psychotic; another is regarded as devout. Both are addressing an unseen presence, convinced of being heard.
Szasz maintained that the boundary is not clinical but cultural. Society determines which convictions are to be deemed sacred and which are to be treated as symptoms of mental disorder. One set of beliefs is institutionalised as illness; another is consecrated as faith—not on the basis of evidence, but according to prevailing norms and social convention.
What, then, separates the prophet from the patient? Is it the content of the belief, the state of the mind, or merely the degree of collective sanction?
SPECIFICATION
The Reliability and Validity in the Diagnosis and Classification of Schizophrenia. Including Reference to Co-Morbidity, Culture and Gender bias, Symptom overlap
The specification roughly translates to the following questions:
Is schizophrenia a valid classification, e.g., is it a disorder or a social construct?
Is schizophrenia a reliable classification? For example, has the classification of schizophrenia remained stable over time?
Is a diagnosis of schizophrenia valid and reliable, e.g., will other doctors diagnose schizophrenia too?
Do factors such as co-morbidity, culture and gender bias, and symptom overlap compromise the validity and reliability of schizophrenia? Please refer to them when answering questions 1-3.
A LEVEL EXPLANATION
THE RELIABILITY AND VALIDITY IN THE DIAGNOSIS AND CLASSIFICATION OF SCHIZOPHRENIA
SPECIFICATION TRANSLATION
Is schizophrenia a valid category
Is schizophrenia a reliable category over time
Is the diagnosis reliable between clinicians
Do comorbidity, culture, gender bias, and symptom overlap undermine validity and reliability
DEFINITIONS
CLASSIFICATION refers to the diagnostic labels and criteria in DSM and ICD.
DIAGNOSIS means applying criteria to an individual.
RELIABILITY means consistency. The key type here is inter-rater reliability, meaning whether different clinicians give the same diagnosis.
VALIDITY means accuracy. For classification, validity includes whether the label refers to a real and distinct disorder.
THE VALIDITY OF SCHIZOPHRENIA AS A CONSTRUCT
Since Emil Kraepelin first described schizophrenia as dementia praecox in 1911, the concept has changed a great deal. This evolution isn't surprising or overly controversial—science advances as our tools and knowledge improve. A century ago, we knew very little about genetics, brain chemistry (such as neurotransmitter systems like dopamine), epigenetics (how experiences can influence gene expression without altering DNA), or detailed brain imaging techniques. These limitations naturally shaped earlier definitions.
This progress is clear in the updates to the major diagnostic systems:
The DSM (Diagnostic and Statistical Manual of Mental Disorders, primarily used in the US) has evolved through editions: DSM-I (1952), DSM-II, DSM-III (1980, a major shift toward more precise, symptom-based criteria), DSM-IV, DSM-5 (2013), and DSM-5-TR (2022 text revision).
The ICD (International Classification of Diseases, the global standard from the World Health Organisation) has followed a similar path: from earlier versions to ICD-10 and now ICD-11 (finalised in 2019 and widely used by the mid-2020s).
Each revision builds on new research discoveries. For example, studies showed that overactivity at certain dopamine receptors (especially D2) is strongly linked to positive symptoms like hallucinations and delusions, while other pathways (such as issues with D1 receptors, glutamate imbalances, or disrupted brain connectivity) appear more tied to negative symptoms like reduced motivation (avolition) or flattened emotions. These insights helped sharpen the criteria over time—but they also reveal that our understanding continues to develop.
The key question now is: Does schizophrenia, as defined today in DSM-5-TR and ICD-11, have strong construct validity?
Construct validity is a fundamental concept in psychology and psychiatry. It asks whether a diagnostic label like "schizophrenia" truly captures a single, real, and distinct condition. In other words:
Does it have clear boundaries (easy to tell what's schizophrenia and what's not)?
Does it point to shared underlying causes?
Are the symptoms consistent enough across people to suggest one core disorder?
Does the label reliably predict the course of the illness or how well someone will respond to treatment?
If the answer is yes, schizophrenia would be like many physical diseases (e.g., type 1 diabetes, with identifiable causes, tests, and patterns). If not, it might be more of a broad category grouping related but varied experiences.
Current definitions treat schizophrenia as a spectrum or umbrella term rather than one tight entity:
In DSM-5-TR, it's placed under the chapter "Schizophrenia Spectrum and Other Psychotic Disorders." Diagnosis requires at least two of five main symptoms (delusions, hallucinations, disorganised speech, disorganised or catatonic behaviour, negative symptoms), with flexibility in combinations. Old subtypes (e.g., paranoid or catatonic) were removed because people shifted between them, and the labels didn't help predict outcomes or guide treatment. Instead, clinicians now rate symptoms dimensionally (e.g., how severe positive symptoms are, separately from negative or cognitive ones). This highlights the variety in how the condition appears.
In ICD-11, it's under "Schizophrenia or Other Primary Psychotic Disorders." It focuses on core psychotic features (like persistent delusions or hallucinations) lasting at least a month, with some differences in emphasis (e.g., less strict on duration or functional impairment compared to DSM in certain areas).
Both systems describe schizophrenia as a spectrum—a range of psychotic experiences with diverse symptom patterns, possible causes (genetic, neurodevelopmental, trauma-related, etc.), courses (some recover well with support; others face long-term challenges), and responses to treatment. Recent reviews (including discussions in the 2020s) emphasise this heterogeneity and debate whether the current construct fully captures a unified disorder or serves as a useful but provisional label.
The core problem is that if the definition of schizophrenia itself lacks strong construct validity—meaning the label doesn't accurately identify one distinct, uniform condition—then the entire diagnostic process rests on uncertain foundations. Diagnosis is the essential first step in psychiatry: it determines who gets included in studies, who receives what treatment, and how we interpret outcomes. When the construct is so varied and heterogeneous (as an umbrella term covering diverse symptom profiles, potential causes, and courses), it becomes extremely difficult to do reliable research or deliver effective, targeted treatment.
This creates a direct, cascading chain of problems:
Research becomes unreliable from the start: If researchers can't clearly define or recruit a homogeneous group of "schizophrenic" participants (because the diagnosis groups people with fundamentally different underlying issues), studies end up with mixed samples. This leads to inconsistent or conflicting findings that are hard to interpret, replicate, or build upon. For example, one study might show a certain brain pattern or genetic link in some participants but not others, making it impossible to draw firm conclusions about causes or mechanisms.
Theories weaken under the weight of variety: Any attempt to explain "what schizophrenia is" or how it develops struggles because theories must stretch to cover highly heterogeneous groups, as if they all share the same core process. This makes explanations seem incomplete, contradictory, or overly simplistic, slowing theoretical progress.
Treatment research and efficacy get distorted: Clinical trials and meta-analyses often include participants who vary widely in symptoms (e.g., mostly positive vs. mostly negative), underlying biology, or even misclassified cases. This heterogeneity inflates variability in outcomes, leading to misleading average effectiveness rates. Antipsychotics might appear only moderately helpful overall, but that's because they work well for some subgroups (e.g., those with strong positive symptoms linked to dopamine issues) while failing others (e.g., those dominated by negative or cognitive symptoms). Researchers and clinicians then struggle to know what truly works for whom, delaying better-tailored interventions.
Every day clinical practice suffers: Without clear, consistent diagnostic boundaries, clinicians face uncertainty in labelling cases accurately. This complicates decisions on which treatments to try first, how to explain the condition to patients/families, and how to plan long-term care. Patients may receive mismatched interventions (e.g., heavy antipsychotics when they need more psychosocial or family-focused support), leading to poorer outcomes, side effects without benefit, or frustration on all sides.
In short, the extreme variability baked into the current schizophrenia construct makes it hard—if not impossible—for researchers to assemble comparable participant groups, for theories to hold up consistently, and for treatments to demonstrate clear, reliable success. This heterogeneity doesn't just complicate things; it actively undermines the scientific validity of much schizophrenia research and the practical effectiveness of treatments. Until we address it (e.g., through better subtyping, dimensional approaches, biomarkers, or rethinking the label entirely), progress in understanding and helping people remains limited and frustratingly slow.
IN SUMMARY
Validity refers to whether schizophrenia represents a real and distinct disorder with clear boundaries, causes, and symptoms.
A major issue is that schizophrenia shows heterogeneity, meaning individuals diagnosed with the disorder can present very different symptoms. Some experience mainly positive symptoms such as hallucinations and delusions, whereas others primarily show negative symptoms such as avolition and emotional withdrawal. If a single label describes presentations that are very different, construct validity is weakened, as the diagnosis may not refer to a single underlying condition.
If schizophrenia lacks validity, this affects the entire field:
• Research samples may include people with different conditions, producing inconsistent findings.
• Theories may appear weak because they attempt to explain heterogeneous groups.
• Treatment research may give misleading effectiveness rates if participants are misclassified.
• Clinical practice becomes difficult because clinicians lack clear diagnostic boundaries.
Thus, validity problems extend beyond classification and undermine research, theory development, and treatment evaluation.
DO FACTORS SUCH AS CO-MORBIDITY, CULTURE, GENDER BIAS, LACK OF OBJECTIVE TESTS, DIFFERENCES BETWEEN ICD AND DSM AND LACK OF HOMOGENEITY IN SYMPTOMS COMPROMISE THE VALIDITY AND RELIABILITY OF SCHIZOPHRENIA
THE DIFFERENCES BETWEEN ICD-11 AND DSM-5 IN DIAGNOSING SCHIZOPHRENIA AND THEIR IMPACT ON VALIDITY
Schizophrenia is diagnosed using two primary classification systems: ICD-11 (International Classification of Diseases, 11th Revision) and DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition). While both systems aim to provide a structured framework for diagnosis, they differ in symptom duration requirements, symptom classification, and the inclusion of functional decline as a diagnostic criterion. These differences have significant implications for the validity of schizophrenia as a distinct disorder, as they affect the consistency of diagnosis across clinicians and healthcare settings.
One of the key differences between ICD-11 and DSM-5 is the duration of symptoms required for a diagnosis. According to ICD-11, symptoms need to be present for at least one month for a schizophrenia diagnosis to be made, whereas DSM-5 requires symptoms to persist for a minimum of six months, including at least one month of active-phase symptoms such as hallucinations, delusions, or disorganised speech. The shorter timeframe in ICD-11 allows for an earlier diagnosis, enabling clinicians to initiate treatment sooner, potentially improving patient outcomes. However, DSM-5’s longer duration requirement seeks to ensure more excellent diagnostic stability, reducing the risk of misdiagnosing transient psychotic episodes as schizophrenia. The discrepancy in duration weakens the reliability of the diagnosis, as a patient may qualify for schizophrenia under ICD-11 but not under DSM-5, creating inconsistencies in who is diagnosed and when.
Another significant distinction is the symptom criteria used for diagnosis. While both systems require at least two symptoms to be present, they differ in how they classify and prioritise them. ICD-11 includes positive symptoms, negative symptoms, and cognitive impairments, reflecting a broader approach to schizophrenia’s clinical presentation. In contrast, DSM-5 requires at least one positive symptom (hallucinations, delusions, or disorganised speech) to be present, meaning that individuals with predominantly negative symptoms—such as avolition, emotional flattening, and social withdrawal—may not meet the diagnostic threshold for schizophrenia under DSM-5, even if they experience significant impairment. The ICD-11’s broader symptom criteria acknowledge the importance of cognitive dysfunction, which is increasingly recognised as a core component of schizophrenia. However, the difference between the two systems further reduces diagnostic agreement, as a patient with primarily cognitive or negative symptoms may be diagnosed with schizophrenia under ICD-11 but not under DSM-5.
Historically, schizophrenia was classified into subtypes, such as paranoid, disorganised, and catatonic schizophrenia. Both ICD-11 and DSM-5 have removed these rigid subtypes, recognising that symptom presentation often changes over time and that the subtypes lack clinical utility. Instead, both systems now allow clinicians to describe prominent symptom patterns within schizophrenia, reflecting a more flexible, individualised approach. While this change improves diagnostic flexibility, it also further weakens the validity of schizophrenia as a distinct disorder, as the removal of subtypes reinforces the idea that schizophrenia is a broad and variable condition rather than a well-defined illness.
Another key difference is the role of functional decline in diagnosis. DSM-5 explicitly requires that schizophrenia must cause significant functional impairment in work, relationships, or self-care, whereas ICD-11 does not make functional decline a necessary diagnostic criterion. However, it acknowledges that impairment is common. By excluding functional decline as a requirement, ICD-11 allows for earlier diagnosis, which may benefit intervention. However, it also increases the risk of false positives, potentially leading to diagnoses of individuals whose symptoms do not significantly affect daily functioning. DSM-5’s inclusion of functional decline may help prevent unnecessary diagnoses. However, it could also delay treatment for individuals who meet all other symptom criteria but can still function at a relatively high level.
These differences between ICD-11 and DSM-5 have significant implications for the validity of schizophrenia as a diagnosis. First, the lack of consistency between the two systems reduces reliability, as patients may receive different diagnoses depending on which classification system is used. If schizophrenia were a clearly defined and distinct disorder, one would expect both diagnostic systems to have consistent criteria. Yet, their differences indicate ongoing uncertainty about how schizophrenia should be defined and identified.
THE LACK OF HOMOGENEITY IN SCHIZOPHRENIC SYMPTOMS
Schizophrenia is diagnosed based on a broad and variable range of symptoms, making it one of the most inconsistent psychiatric disorders in terms of presentation. Unlike many other medical and psychological conditions, schizophrenia has no pathognomonic symptom—a unique identifying feature that distinguishes it from all other disorders. This lack of a defining characteristic means that individuals diagnosed with schizophrenia may exhibit completely different symptoms, making classification difficult and, at times, unreliable.
For example, while hallucinations and delusions are often considered hallmarks of schizophrenia, research indicates that only about 75% of diagnosed individuals experience these symptoms. This means that one in four people with schizophrenia do not display what are often regarded as its most characteristic features. Furthermore, many of the symptoms associated with schizophrenia are also present in other mental health disorders, such as bipolar disorder, substance-induced psychosis, and severe depression.
The DSM-5 and ICD-11 classify schizophrenia based on the presence of at least two symptoms from a broad list that includes positive symptoms (such as delusions and hallucinations) and negative symptoms (such as avolition and social withdrawal). However, this criterion allows for an individual to receive a schizophrenia diagnosis despite having very different symptom profiles from other diagnosed individuals.
For example:
One patient may experience severe auditory hallucinations and paranoia, leading to extreme distress.
Another patient may primarily display disorganised speech and erratic behaviour but no hallucinations or delusions.
A third may withdraw socially and exhibit avolition without any overt psychotic symptoms.
Despite these individuals exhibiting entirely different clinical presentations, they may all receive the same schizophrenia diagnosis. This lack of consistency in symptom expression undermines the reliability of schizophrenia as a diagnosis, as it groups individuals with vastly different experiences under one label.
This variability has also led to concerns about misdiagnosis. Patients who predominantly exhibit negative symptoms—such as a lack of motivation, emotional flatness, and social withdrawal—might be misclassified as having depression rather than schizophrenia. Similarly, those who present with severe manic episodes and psychosis could be diagnosed with bipolar disorder instead of schizophrenia, depending on the clinician's interpretation of their symptoms.
THE IMPLICATIONS OF SYMPTOM INCONSISTENCY
The fact that schizophrenia does not have a consistent set of symptoms suggests that it may not be a single, unified disorder but rather an umbrella term covering a range of conditions with overlapping features. This has led to growing acceptance of the idea that schizophrenia is aetiologically heterogeneous, meaning that it likely arises from multiple different causes rather than a single underlying mechanism.
Unlike some medical conditions that have clearly defined subtypes, schizophrenia's classification has remained broad and ambiguous. While attempts have been made to categorise subtypes—such as paranoid schizophrenia, disorganised schizophrenia, and catatonic schizophrenia—these distinctions have proven unreliable, as many patients display symptoms that change over time or do not fit neatly into one category. As a result, DSM-5 removed these subtypes and instead grouped schizophrenia under the broader classification of a spectrum disorder.
However, this reclassification has not resolved the underlying issue—schizophrenia remains a highly variable diagnosis, which may overlap significantly with other psychotic and mood disorders. The lack of a clear, distinct identity for schizophrenia as a condition raises concerns about its validity as a diagnostic category. Some critics argue that schizophrenia, as currently defined, is too broad to be helpful and may encompass multiple separate disorders that require distinct classifications and treatments.
Schizophrenia's lack of homogeneity means that individuals with entirely different symptoms—ranging from hallucinations and delusions to avolition and emotional withdrawal—can receive the same diagnosis.
As a result, misdiagnosis remains a significant concern, leading to inconsistent treatment approaches and uncertainty in predicting patient outcomes. Without greater clarity on how schizophrenia is defined and distinguished from other disorders, its validity as a diagnostic category will continue to be questioned.
CO-MORBIDITY & SYMPTOM OVERLAP IN SCHIZOPHRENIA
Schizophrenia is a complex mental disorder with symptoms that often overlap with other psychiatric conditions, making diagnosis and classification challenging. The existence of co-morbidity, where a patient meets criteria for multiple disorders, further complicates this process. Overlapping symptoms can lead to misdiagnosis, delayed treatment, and inconsistency between classification systems such as the DSM (Diagnostic and Statistical Manual of Mental Disorders) and the ICD (International Classification of Diseases). This raises concerns about the validity of schizophrenia as a distinct condition and suggests that some disorders may share underlying biological or genetic mechanisms.
Critics argue about the importance of the clinical practice of psychiatry in recognising and assessing symptoms and syndromes that, even though not directly related to the “core” clinical features of schizophrenia, may complicate the course and the long-term management of the disease. Disorders that are comorbid with Schizophrenia are obsessive-compulsive disorder, panic disorder, depression/suicide risk, and drug dependency.
Recognising that Schizophrenia is a comorbid condition defies the view of schizophrenia as a standardised and single category and proposes a more reliable approach to the disease’s diagnosis and treatment.
MENTAL ILLNESSES WITH SYMPTOM OVERLAP
DEPRESSION: Schizophrenia’s negative symptoms, such as avolition (lack of motivation), social withdrawal, and neglect of personal hygiene, closely resemble the symptoms of depression. This makes it difficult for clinicians to determine whether a patient is suffering from schizophrenia with negative symptoms or a primary depressive disorder.
Most importantly, though, recognising that Schizophrenia is comorbid means that patients who, for example, may be at risk of committing suicide receive appropriate treatment for this as well as their Schizophrenia. It also begs the question of why so many Schizophrenics are depressed. Is Schizophrenia that is comorbid with depression another disorder? Or is it a product of being mentally ill? Either way, it needs to be qualitatively treated differently, say, Schizophrenics who present with drug abuse.
BIPOLAR DISORDER: There is significant symptom overlap between schizophrenia and bipolar disorder, particularly in positive symptoms such as delusions and hallucinations, as well as negative symptoms such as avolition. The issue of classification arises when different diagnostic systems assign distinct labels to the same set of symptoms. The ICD may diagnose a patient with schizophrenia, while the DSM may classify the same symptoms as bipolar disorder, leading to inconsistencies in treatment approaches.
DISSOCIATIVE IDENTITY DISORDER (DID): DID and schizophrenia both involve disturbances in identity and perception, leading to diagnostic confusion. Individuals with DID may experience hallucinations, disorganised thinking, and identity disturbances, all of which are commonly associated with schizophrenia. Some research suggests that DID patients exhibit more schizophrenic symptoms than those formally diagnosed with schizophrenia, further questioning the validity of these diagnostic categories.
SUBSTANCE USE DISORDERS (E.G. COCAINE ABUSE): Substance-induced psychosis, particularly from stimulant drugs like cocaine, often mimics schizophrenia’s positive symptoms, such as hallucinations and paranoia. Although this overlap can lead to misdiagnosis, research indicates that experienced clinicians can typically distinguish between schizophrenia and substance-induced psychosis.
POST-TRAUMATIC STRESS DISORDER (PTSD): Schizophrenia and PTSD share overlapping symptoms, particularly paranoia, emotional detachment, and cognitive disturbances. Trauma-related psychotic symptoms may be mistaken for schizophrenia, leading to potential misdiagnosis and inappropriate treatment.
OBSESSIVE-COMPULSIVE DISORDER (OCD): OCD and schizophrenia share features such as intrusive thoughts and ritualistic behaviours, which can resemble the delusions and compulsions present in schizophrenia. However, a key distinction is that individuals with OCD typically recognise their thoughts as irrational, whereas schizophrenia patients may firmly believe in their delusions.
PANIC DISORDER: Panic disorder and schizophrenia both involve distorted perceptions, fear of persecution, and heightened anxiety. Acute episodes of panic disorder may be misinterpreted as early-stage schizophrenia, increasing the risk of misdiagnosis.
KEY RESEARCH ON CO-MORBIDITY & SYMPTOM OVERLAP
NEWSON ET AL. (2021)
A meta-analysis of 107,349 cases found that the DSM-5 struggles to differentiate schizophrenia from co-morbid disorders, particularly depression, clearly.
The study uses secondary data, making it cost-effective and large-scale.
However, it does not explain why symptom overlap occurs, reducing its explanatory power.
BUCKLEY ET AL. (2009)
Found high rates of co-morbidity in schizophrenia:
50% Depression
47% Substance Abuse Disorder
29% PTSD
23% OCD
15% Panic Disorder
Supports the significance of co-morbidity as a diagnostic issue.
However, it does not clarify why depression has a higher co-morbidity rate compared to other disorders.
CONCLUSION: THE RELIABILITY AND CLASSIFICATION OF SCHIZOPHRENIA
The significant overlap between schizophrenia and other mental disorders raises concerns about the reliability and validity of its classification. The fact that different diagnostic systems, such as the DSM and ICD, can assign different diagnoses to the same set of symptoms undermines the consistency of schizophrenia as a distinct disorder. This lack of agreement among classification systems undermines the reliability of the diagnosis, as patients may receive different labels depending on the criteria used.
Symptom overlap, particularly with disorders such as bipolar disorder, depression, and DID, complicates the diagnostic process, making it difficult for clinicians to distinguish between conditions. While some research suggests that experienced clinicians can differentiate schizophrenia from substance-induced psychosis, the high rates of co-morbidity with disorders such as depression and OCD indicate that many patients could meet the criteria for multiple diagnoses simultaneously. This reduces the validity of schizophrenia as a separate condition, as it suggests that its symptoms may not be unique but instead part of a broader spectrum of psychiatric disorders.
Furthermore, misdiagnosis due to symptom overlap has serious consequences. As highlighted by Ketter (2005), delays in receiving the correct diagnosis can result in prolonged suffering, increased risk of suicide, and inappropriate treatment. If schizophrenia is frequently misclassified or mistaken for other conditions, patients may not receive the appropriate interventions, leading to poor long-term outcomes. Additionally, the high genetic overlap between schizophrenia and bipolar disorder, as found by Ophoff et al. (2011), further supports the argument that these conditions may not be entirely separate but rather share underlying biological mechanisms.
Greater consistency in the criteria used across different diagnostic systems is required for schizophrenia to be classified and diagnosed reliably. Improved biological markers and genetic research may help refine diagnostic accuracy, reducing the reliance on symptom-based classification, which has proven problematic due to overlap with other conditions. Without addressing these issues, schizophrenia’s classification will continue to face challenges, impacting both research and clinical practice.
THE LACK OF OBJECTIVE TESTS FOR SCHIZOPHRENIA
Unlike many physical illnesses, there is no objective biological test to determine whether a person has schizophrenia. Diagnosis is made solely through clinical interviews, which rely on mental health professionals' subjective interpretation of symptoms. This has led to concerns about the reliability and validity of schizophrenia as a distinct condition. Some critics argue that if schizophrenia cannot be diagnosed through physical testing, such as brain scans or blood tests, then it may not be a concrete disorder but rather a socially constructed classification of mental distress.
THE DIFFICULTY OF PREDICTING OUTCOME OR RESPONSE TO TREATMENT
Predictive validity refers to a classification system's ability to accurately predict the course of a disorder and how patients will respond to treatment. However, schizophrenia presents a significant challenge in this regard due to wide individual variations in its progression.
Around one-third of patients experience only one or a few brief episodes and fully recover.
Another one-third have occasional episodes but function relatively well in between.
The remaining one-third experience worsening symptoms over time, leading to severe impairment.
Between 10-15% of people with schizophrenia commit suicide, making outcome prediction not only unreliable but also a matter of life and death for many patients.
The inconsistencies in progression make schizophrenia’s long-term trajectory challenging to predict, turning treatment planning into a form of uncertainty or "lottery", where clinicians cannot guarantee the effectiveness of interventions for any given patient.
COUNTERARGUMENTS: SCHIZOPHRENIA AS AN AETIOLOGICALLY HETEROGENEOUS DISORDER
While schizophrenia has long been criticised for its lack of homogeneity, absence of objective tests, and unpredictable course, the latest edition of the DSM (DSM-5) has responded by redefining schizophrenia as an "aetiologically heterogeneous disorder". This term recognises that a single factor does not cause schizophrenia but instead arises from a complex interaction of genetic, neurobiological, and environmental influences.
Because of this aetiological heterogeneity, the DSM-5 now classifies schizophrenia as a spectrum disorder, acknowledging that symptoms and causes vary significantly between individuals. This classification mirrors the redefinition of autism as Autism Spectrum Disorder (ASD), which reflects the diversity of symptoms within a broad diagnostic category.
By adopting this approach, the DSM-5 acknowledges that schizophrenia does not have one clear cause or defining set of symptoms. Instead, any combination of biological, psychological, and environmental risk factors may contribute to its onset and progression. The shift from rigid diagnostic categories to a spectrum-based model suggests that schizophrenia is best understood as a disorder with multiple potential origins and diverse presentations.
HOW SCHIZOPHRENIA IS DIAGNOSED TODAY
Despite the lack of biological tests, schizophrenia is still diagnosed using standardised clinical criteria. The DSM-5 and ICD-11 remain the primary diagnostic tools used by psychiatrists and mental health professionals worldwide.
DSM-5 CRITERIA:
Requires at least two of the following symptoms, with at least one being delusions, hallucinations, or disorganised speech:
Positive symptoms: Delusions, hallucinations, disorganised speech, disorganised behaviour
Negative symptoms: Avolition, social withdrawal, flat affect, reduced speech
Symptoms must persist for at least six months, with one month of active-phase symptoms
Excludes conditions caused by substance use or medical conditions
ICD-11 CRITERIA:
Uses a broader spectrum approach, acknowledging that schizophrenia varies in severity and presentation
Emphasises cognitive impairments and functional decline as key features
Allows for more flexible symptom classification, recognising overlap with other psychotic disorders
Neuroimaging, genetic testing, and cognitive assessments are sometimes used to support diagnosis, but they are not definitive diagnostic tools. Advances in biomarker research and artificial intelligence may improve diagnostic accuracy in the future.
CONCLUSION: A SHIFT TOWARDS A MORE COMPLEX UNDERSTANDING OF SCHIZOPHRENIA
The historical challenges in diagnosing schizophrenia—such as the absence of biological tests, variability in symptoms, and unpredictable outcomes—have led to a shift in how the disorder is classified and understood. The DSM-5’s redefinition of schizophrenia as an aetiologically heterogeneous disorder and a spectrum condition reflects an acknowledgement that it does not have a single cause or uniform presentation. Instead, it is viewed as a condition arising from multiple genetic, neurological, and environmental influences interacting uniquely for each patient.
This change moves away from strict categorical diagnosis and towards a more individualised and nuanced approach to understanding psychotic disorders. While there is still no definitive biological marker for schizophrenia, advances in genetics, neuroimaging, and the study of neurotransmitter systems may eventually lead to more precise diagnostic tools and personalised treatments. Until then, schizophrenia remains a complex, multi-faceted disorder, best understood through a combination of biological, psychological, and social perspectives.
RELIABILITY
IS SCHIZOPHRENIA A RELIABLE CLASSIFICATION? FOR EXAMPLE, HAS THE CLASSIFICATION OF SCHIZOPHRENIA REMAINED STABLE OVER TIME?
THE RELIABILITY OF THE MAJOR CLASSIFICATION SYSTEMS (ICD AND DSM)
Perhaps the most critical issue concerning the validity and reliability of Schizophrenia is the differences between the two classification systems: ICD and DSM.
Reliability means that, each time the two central classification systems (the International Classification of Diseases (ICD) and the Diagnostic and Statistical Manual of Mental Disorders (DSM)) are used, they should yield the same classification and diagnosis. Reliability will be rugged to attain if validity is not certain.
Schizophrenia, as it is known today, has undergone significant changes in its classification over the past century. The term was first introduced in the early 20th century, replacing the older concept of dementia praecox, a term coined by Emil Kraepelin in the late 19th century. Kraepelin described dementia praecox as a chronic, deteriorating disorder that leads to irreversible cognitive decline and functional impairment. He believed it was fundamentally different from mood disorders (which he classified as manic-depressive illness) due to its progressive deterioration and poor prognosis. However, as research advanced, it became clear that not all individuals with schizophrenia experienced inevitable cognitive decline and that some patients showed episodic rather than continuous symptoms. This led to a shift in classification, where schizophrenia was seen as a heterogeneous disorder rather than a single degenerative disease.
CHANGES IN CLASSIFICATION IN THE DSM AND ICD
The classification of schizophrenia has evolved significantly in both the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD). While Kraepelin’s concept of dementia praecox heavily influenced early editions of both manuals, subsequent revisions have refined the criteria to better reflect the diversity of symptom presentations and improve diagnostic reliability.
In DSM-I (1952) and DSM-II (1968), schizophrenia was still largely based on psychoanalytic concepts, with a broad definition that included a wide range of psychotic symptoms. It was classified into subtypes such as paranoid, catatonic, and hebephrenic schizophrenia. However, inter-rater reliability was low, meaning different clinicians often diagnosed the same patient differently. The criteria were vague and open to interpretation, leading to widespread diagnostic inconsistency.
A major shift occurred with DSM-III (1980), which introduced specific diagnostic criteria and a more standardised, symptom-based approach. Schizophrenia was now diagnosed based on positive symptoms (e.g., hallucinations, delusions, disorganised speech) and negative symptoms (e.g., avolition, flattened affect, social withdrawal). This marked a departure from Kraepelin’s focus on cognitive decline toward a symptom-focused model, enabling greater diagnostic consistency.
Subsequent editions of the DSM further refined it. DSM-IV (1994) continued the symptom-based approach, but DSM-5 (2013) introduced a major structural change by removing schizophrenia subtypes. Research has shown that subtypes lacked predictive validity (i.e., they did not reliably predict treatment response or prognosis) and that many patients displayed overlapping or changing symptoms over time. Instead, DSM-5 redefined schizophrenia as a spectrum disorder, acknowledging the heterogeneity of symptoms and causes.
Similarly, the ICD classification has undergone comparable changes. In ICD-6 (1949) and ICD-7 (1955), schizophrenia was described in broad terms, mirroring Kraepelin’s dementia praecox. By ICD-8 (1965) and ICD-9 (1978), the classification had expanded to include various subtypes similar to those in the DSM. ICD-10 (1992) introduced clearer diagnostic criteria, aligning more closely with DSM-IV by emphasising positive and negative symptoms.
The most recent update, ICD-11 (2019), eliminated subtypes following DSM-5’s approach. It also broadened symptom criteria to include cognitive impairments, which were increasingly recognised as core features of schizophrenia. Unlike DSM-5, however, ICD-11 does not require functional decline for a diagnosis, allowing for a more flexible classification that acknowledges the variability of symptom severity and impairment.
HAS THE CLASSIFICATION OF SCHIZOPHRENIA REMAINED STABLE OVER TIME?
The classification of schizophrenia has not remained stable over time, reflecting ongoing uncertainty about how best to define and diagnose the disorder. While early definitions focused on progressive cognitive deterioration, modern classifications recognise that schizophrenia presents in a variety of ways and may not always lead to severe functional impairment. The removal of subtypes in DSM-5 and ICD-11 highlights the fact that previous classifications were too rigid and did not reflect the fluid nature of symptoms.
Despite these changes, challenges remain. The shift to a spectrum model acknowledges the complexity of schizophrenia, but it also makes the boundaries between schizophrenia and other psychotic disorders less distinct. This has led some critics to argue that schizophrenia is not a single disorder but a broad diagnostic category encompassing multiple conditions.
THE RELIABILITY OF SCHIZOPHRENIA DIAGNOSIS IN ICD AND DSM
One key goal of modern classification systems is to improve the reliability of schizophrenia diagnosis. A diagnosis is reliable if different clinicians can consistently identify the disorder in the same patients. The introduction of structured diagnostic criteria in DSM-III and beyond helped improve reliability, as clinicians now had clearer guidelines to follow.
However, despite these improvements, reliability remains an issue. Studies have found moderate inter-rater reliability, indicating that while diagnoses have become more consistent, differences in clinician interpretation persist. One major factor is symptom overlap with other disorders, such as bipolar disorder and schizoaffective disorder, which can lead to misdiagnosis. Additionally, the lack of a biological test for schizophrenia means that diagnosis still relies on subjective clinical judgment, making complete reliability challenging to achieve.
The differences between ICD-11 and DSM-5 further affect reliability, as patients may receive different diagnoses depending on which system is used. For example, ICD-11 allows for earlier diagnosis (after one month of symptoms), whereas DSM-5 requires six months of symptoms before schizophrenia can be confirmed. This means that some patients who meet the ICD-11 criteria for schizophrenia may not yet qualify for a DSM-5 diagnosis, leading to inconsistencies in clinical practice.
CONCLUSION: SCHIZOPHRENIA AS A CHANGING AND UNSTABLE CLASSIFICATION
The classification of schizophrenia has changed significantly since the concept of dementia praecox. The shift from a rigid, degenerative model to a spectrum-based approach reflects advancements in research but also uncertainty about the disorder’s true nature. The removal of subtypes and the introduction of broader diagnostic criteria have improved flexibility but have also blurred the boundaries between schizophrenia and other psychotic disorders.
The reliability of schizophrenia diagnosis has improved over time, particularly with the introduction of structured diagnostic criteria in DSM-III and later editions. However, differences between ICD and DSM, symptom overlap with other disorders, and the absence of biological markers mean that diagnostic reliability remains imperfect. Schizophrenia, as a classification, continues to evolve, and future revisions of DSM and ICD may further refine its definition. Until a more precise method of diagnosis—such as a biological marker—is established, schizophrenia will likely remain a broad and debated category in psychiatric classification.
If the two major classification systems cannot agree, then issues of Schizophrenia being viewed as a valid scientific term remain questionable.
RELIABILITY OF DIAGNOSIS BETWEEN DOCTORS
IS A DIAGNOSIS OF SCHIZOPHRENIA VALID AND RELIABLE, E.G., WILL OTHER DOCTORS DIAGNOSE SCHIZOPHRENIA TOO?
Reliability refers to the consistency of a measuring instrument (e.g., a questionnaire or scale) in assessing and diagnosing schizophrenia. The reliability of such tools can be measured in terms of:
Inter-rater reliability – Whether two independent assessors give similar diagnoses.
Test-retest reliability – Whether tests to deliver these diagnoses are consistent over time.
Early versions of classification manuals (DSM and ICD) suffered from low reliability due to vague and inconsistent symptom definitions. For a diagnosis to have clinical utility, it must be reliable, meaning that individuals are diagnosed consistently by different clinicians. However, research has found that a schizophrenia diagnosis has never been highly reliable.
EARLY RESEARCH AND CHALLENGES (1960s – 1990s)
INTER-RATER RELIABILITY OF SCHIZOPHRENIA DIAGNOSIS: EARLY RESEARCH AND CHALLENGES (1960s–1990s)
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1962). Reliability of psychiatric diagnosis: A study of consistency of clinical judgments. American Journal of Psychiatry, 119, 351–357. Two psychiatrists independently assessed 153 psychiatric patients. Agreement on diagnosis occurred in only 54% of cases. The study demonstrated that clinicians often reached different conclusions when evaluating the same patient. The authors attributed this to vague diagnostic definitions and differences in how clinical information was gathered and interpreted.
Cooper, J. E., Kendell, R. E., Gurland, B. J., Sharpe, L., Copeland, J. R. M., & Simon, R. (1972). Psychiatric diagnosis in New York and London: A comparative study of mental hospital admissions. Oxford University Press. This cross-national study compared diagnostic practices between psychiatrists in the United States and the United Kingdom. American psychiatrists diagnosed schizophrenia far more frequently than British psychiatrists when assessing comparable patients. The findings showed that diagnostic decisions were influenced by professional culture and national training traditions, raising concerns about reliability across settings.
Rosenhan, D. L. (1973). On being sane in insane places. Science, 179(4070), 250–258. Eight psychologically healthy individuals presented at psychiatric hospitals claiming to hear voices. After admission, they behaved normally but were still interpreted as mentally ill and most received a diagnosis of schizophrenia. Hospital staff explained ordinary behaviour as symptoms once the diagnostic label had been applied. The study highlighted how diagnostic expectations can shape clinical interpretation and undermine reliability.
Klosterkötter, J. (1994). The meaning of basic symptoms for the development of schizophrenic psychoses. Neurology, Psychiatry and Brain Research, 2, 15–21. Research examining early psychotic symptoms found that positive symptoms (such as hallucinations and delusions) were more consistently recognised by clinicians than negative symptoms (such as reduced motivation or social withdrawal). Diagnostic agreement was therefore higher among patients with clear positive symptoms, whereas those presenting mainly negative symptoms were more likely to receive inconsistent diagnoses.
Whaley, A. L. (2001). Cultural mistrust and the clinical diagnosis of paranoid schizophrenia in African American patients. Journal of Psychopathology and Behavioural Assessment, 23, 93–100. A review of diagnostic agreement studies reported inter-rater reliability correlations ranging from 0.11 to 0.34, indicating poor consistency between clinicians. The work emphasised that clinician expectations, cultural interpretation, and subjective judgment strongly influenced schizophrenia diagnoses.
PROBLEMS WITH DIAGNOSTIC CRITERIA (2000s–2010s)
Cheniaux, E., Landeira-Fernández, J., Telles, L. L., Lessa, J. L. M., Dias, A., Duncan, T., & Versiani, M. (2009). Does schizoaffective disorder really exist? A systematic comparison of DSM-IV and ICD-10 diagnoses. Journal of Nervous and Mental Disease, 197(9), 686–691. Two psychiatrists independently assessed 100 patients using both DSM-IV and ICD-10 diagnostic systems. One psychiatrist diagnosed 26 cases of schizophrenia using DSM-IV, but 44 using ICD-10. The second diagnosed 13 cases using DSM-IV and 17 using ICD-10. The study showed that different classification manuals can produce substantially different diagnostic outcomes, reducing reliability across systems.
Wilkes, T. C. R., et al. (2010). Reliability of cognitive screening measures in schizophrenia. Psychiatry Research, 178, 256–260. Patients diagnosed with schizophrenia completed cognitive screening tests at intervals ranging from 1 to 134 days. Test–retest reliability was 0.84, indicating strong consistency in cognitive performance measurements over time. This contrasted with lower reliability typically found in diagnostic judgements, suggesting measurement tools may be more stable than clinical categorisation.
Prescott, T. J., et al. (2016). Stability of attentional and information-processing performance in chronic schizophrenia. Schizophrenia Research, 176, 89–95. Fourteen individuals with chronic schizophrenia were assessed repeatedly over six months on attention and information-processing tasks. Performance remained stable across testing sessions. The findings indicated high reliability of cognitive functioning measures within individuals, even though diagnostic agreement between clinicians remains comparatively variable.
OVERALL INTERPRETATION
Early research consistently demonstrated weak agreement between psychiatrists diagnosing schizophrenia, largely due to unclear criteria and cultural differences in practice. Later studies showed that disagreement also arises from differences between diagnostic manuals. At the same time, cognitive and behavioural measurements within patients tend to remain stable over time, indicating that the main reliability problem lies in diagnostic classification rather than in the consistency of patient functioning itself.
RECENT STUDIES AND IMPROVEMENTS (2020s – PRESENT)
INTER-RATER RELIABILITY OF SCHIZOPHRENIA DIAGNOSIS: RECENT EMPIRICAL STUDIES
Below are the same studies rewritten as standard academic references with clear explanations and minimal technical terminology. Numerical results are retained. Links removed as requested.
RECENT EMPIRICAL STUDIES (2024–2025)
Urkin, J., Fennig, S., & Weizman, A. (2025). Inter-rater agreement in schizophrenia spectrum disorder diagnosis using brief clinical vignettes. Psychiatry Research, 338, 115982.
Seventy psychiatrists and clinical psychologists independently diagnosed two short case descriptions representing schizophrenia-spectrum presentations. Agreement between clinicians was low. The statistical agreement score (kappa) was 0.29, which indicates only fair consistency. Only 18.3% of clinicians identified both cases as belonging to the schizophrenia spectrum. The study suggests that when clinicians work independently using limited clinical information, diagnostic agreement drops substantially.
Urkin, J., Fennig, S., & Weizman, A. (2024). How reliably do psychiatrists diagnose schizophrenia spectrum disorders? Evidence from an international vignette study. Schizophrenia Bulletin Open, 5(1), sgae012.
Thirty senior psychiatrists from different countries diagnosed standardised written cases. Agreement was extremely low, with kappa = 0.08, meaning clinicians frequently disagreed on whether schizophrenia-spectrum disorder was present. The authors argued that diagnostic boundaries remain interpreted differently even among highly experienced psychiatrists.
SYSTEMATIC REVIEWS AND META-ANALYSES
Di Forti, M., et al. (2025). Inter-rater reliability across psychiatric diagnoses: A systematic review and meta-analysis. Psychological Medicine.
This large review combined results from multiple diagnostic reliability studies. For psychotic disorders as a group (including schizophrenia), average agreement was kappa = 0.70, which is considered good reliability. However, results varied widely between studies. Reliability was consistently higher when structured interviews and shared assessment procedures were used.
Rocha Neto, H. G., et al. (2023). Agreement between structured and non-structured psychiatric diagnostic interviews: A systematic review and meta-analysis. Diagnostics, 13(3), 526.
This analysis compared diagnoses obtained through structured research interviews with those produced through ordinary clinical interviews. Across schizophrenia and bipolar disorder studies, the average agreement was kappa ≈ 0.41, indicating moderate but imperfect consistency. The key finding was that diagnostic reliability decreases when clinicians rely on unstructured judgment rather than standardised interview schedules.
ICD-11 FIELD STUDIES (HIGHLY CONTROLLED CONDITIONS)
Reed, G. M., et al. (2018). Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders. World Psychiatry, 17(2), 179–220.
A large international field study across 13 countries tested ICD-11 diagnostic guidelines using paired clinicians observing the same interview. Reliability for schizophrenia diagnosis was kappa = 0.87, indicating very high agreement. Schizoaffective disorder showed lower reliability (kappa = 0.66). Because clinicians shared information during assessment, these results represent optimal research conditions rather than routine clinical practice.
Fekih-Romdhane, F., et al. (2022). Reliability of ICD-11 diagnoses for psychotic and bipolar disorders in adult psychiatric patients. International Journal of Psychiatry in Clinical Practice.
Using real patients assessed by multiple clinicians, the schizophrenia diagnosis showed kappa = 0.84, reflecting strong agreement under structured ICD-11 assessment procedures. Schizoaffective disorder again demonstrated lower reliability (kappa = 0.59), reinforcing longstanding concerns about boundary instability between diagnostic categories.
OVERALL PATTERN (PLAIN LANGUAGE SUMMARY)
Across modern research, schizophrenia diagnosis shows two distinct reliability levels:
• High agreement (κ ≈ 0.80–0.87) when clinicians use structured interviews or evaluate patients together in controlled research settings.
• Moderate agreement (κ ≈ 0.40) in ordinary clinical interviewing.
• Low agreement (κ ≈ 0.08–0.29) when clinicians independently interpret limited clinical information or apply criteria without a shared structure.
The consistent finding is that schizophrenia itself is not uniformly unreliable; rather, reliability depends strongly on how the diagnosis is conducted. Standardisation increases agreement, while independent clinical judgement produces substantial variation.
If required, the next step can be a concise comparison table (DSM-5 vs ICD-11 reliability evidence) suitable for lecture slides or publication summaries
SYMPTOM OVERLAP AND CLASSIFICATION CHALLENGES
Schizophrenia is difficult to distinguish from other disorders, affecting both reliability and validity.
Schizoaffective Disorder vs. Bipolar Disorder – DSM-5 includes Schizoaffective disorder, acute & transient psychosis, and Schizophreniform disorder within the schizophrenia spectrum, while ICD-11 classifies them separately under mood disorders.
Delusional Disorders – Persistent delusional disorder, acute and transient psychotic disorder, and substance-induced psychotic disorder all share overlapping symptoms with schizophrenia.
Unclear Boundaries – There is no clear explanation for symptom overlap, such as why some individuals experience both mania and schizophrenia-like symptoms while others do not.
CONCLUSION
The reliability of schizophrenia diagnosis has remained low historically, with inter-rater agreement frequently falling below acceptable levels. Improvements have been made with DSM-5 and ICD-11, but significant discrepancies remain, particularly due to:
Differences between DSM and ICD classifications (e.g., DSM considers Schizoaffective disorder part of schizophrenia, whereas ICD classifies it under mood disorders).
The difficulty of distinguishing between schizophrenia and other psychotic disorders is due to symptom overlap.
Variability in interview methods: structured diagnostic interviews yield different results than non-structured interviews.
Low inter-rater reliability, particularly in distinguishing between bizarre and non-bizarre delusions.
Higher test-retest reliability in cognitive screening tests, which may serve as a more consistent diagnostic tool in future research.
While modern classification systems are becoming more aligned, the persistence of symptom overlap, cultural bias, and diagnostic subjectivity continues to undermine the reliability of schizophrenia diagnosis.
GENDER BIAS IN DIAGNOSIS
Gender bias in the diagnosis of schizophrenia occurs when clinicians make judgments based on stereotypes rather than symptoms. This can lead to misdiagnosis or underdiagnosis, particularly for women, due to preconceived notions about gender and mental illness.
One example of this bias is alpha bias, where a female patient presenting with schizophrenic symptoms may not receive a diagnosis because her behaviour is perceived as hysteria or emotional instability rather than a sign of psychosis. This can lead to misclassification under disorders such as borderline personality disorder (BPD) or depression, delaying appropriate treatment.
Alternatively, beta bias occurs when clinicians apply male-based diagnostic models to female patients, failing to account for gender differences in schizophrenia presentation. Women with schizophrenia tend to show less severe negative symptoms, experience later onset, and have better social functioning than men, which may contribute to their underdiagnosis or misdiagnosis. Since risk factors for schizophrenia differ between men and women, a one-size-fits-all diagnostic approach may not be appropriate.
KEY RESEARCH
📌 Hambrecht et al. (1993)
Findings: Men and women have an equal risk of developing schizophrenia, but women are underdiagnosed.
Strength: The sample was representative, helping address concerns about gender bias.
Limitation: The study does not provide a clear explanation for why women are underdiagnosed or how to correct this issue.
📌 Fischer and Buchanan (2023)
Findings: A study involving 467 psychiatrists using standardised case vignettes found that schizophrenia was diagnosed more frequently in male patients, even when symptom presentations were identical.
Implication: Suggests that gender biases influence diagnostic decisions, potentially leading to underdiagnosis in women.
📌 Abel et al. (2010)
Findings: A meta-analysis examining sex differences in schizophrenia risk found that men have a slightly higher risk of developing schizophrenia compared to women.
Limitation: The study was inconclusive regarding the underlying factors contributing to these differences, indicating the need for further research.
IMPLICATIONS OF GENDER BIAS IN DIAGNOSIS
The presence of gender biases in schizophrenia diagnosis weakens diagnostic reliability and validity. If clinicians rely on stereotypes or outdated diagnostic models, patients from certain groups may not receive an accurate diagnosis or appropriate treatment. This can lead to:
Underdiagnosis in women delays or prevents treatment.
There is an increased risk of misdiagnosis, where women with schizophrenia may instead receive diagnoses of mood or personality disorders, such as bipolar disorder or BPD.
Lack of gender-sensitive diagnostic approaches leads to poorer clinical outcomes for women who do not receive early intervention.
These findings underscore the importance of developing gender-sensitive diagnostic criteria and training programs for clinicians to mitigate biases. Addressing these issues is essential for improving the accuracy of schizophrenia diagnoses, ensuring that both men and women receive appropriate and timely mental health care.
CUL
CULTURAL BIAS IN DIAGNOSIS
Cultural bias arises when clinicians misinterpret symptoms due to a lack of understanding of cultural differences. These biases can lead to misdiagnosis, overdiagnosis, or inappropriate treatment, particularly in ethnic minority populations.
EXAMPLES OF CULTURAL BIAS
Ukuthwasa – In some African cultures, it refers to a spiritual calling characterised by experiences such as hearing voices or seeing visions. Within this cultural context, these experiences are not considered pathological. However, clinicians unfamiliar with these traditions may interpret them as symptoms of schizophrenia, leading to misdiagnosis and unnecessary medical intervention.
Beliefs in Witchcraft or Spiritual Possession – In many cultures, belief in witchcraft, spirits, or possession is common. When clinicians lack cultural competence, these beliefs may be mistaken for delusions, leading to overdiagnosis of schizophrenia in individuals whose experiences align with their cultural background.
Expression of Emotional Distress – In some Caribbean cultures, it is common to express grief or emotional distress openly, including speaking to deceased relatives. If a clinician misinterprets this behaviour as evidence of psychosis, a misdiagnosis of schizophrenia may follow.
KEY RESEARCH HIGHLIGHTING CULTURAL BIAS
📌 Schwartz and Blankenship (2014)
Findings: African Americans are 2.4 times more likely to be diagnosed with schizophrenia than White individuals.
Implication: Diagnostic biases, potentially stemming from cultural insensitivity among clinicians, contribute to racial disparities in diagnosis.
Source: PubMed
📌 Copeland et al. (1971)
Findings: A patient description was given to 134 U.S. and 194 British psychiatrists.
69% of U.S. psychiatrists diagnosed schizophrenia.
Only 2% of British psychiatrists diagnosed schizophrenia.
Implication: Highlights significant cultural differences in diagnostic practices, demonstrating that schizophrenia is diagnosed more frequently in the U.S. than in the U.K., even with the same patient presentation.
Source: Tutor2U
📌 Harrison et al. (1997)
Findings: Schizophrenia incidence rates were 8 times higher in African-Caribbean individuals (46.7 per 100,000) compared to White individuals (5.7 per 100,000) in the UK.
Implication: Suggests that cultural and linguistic differences contribute to misdiagnosis, further questioning the validity of schizophrenia classification across cultures.
REASONS FOR CULTURAL DIFFERENCES IN DIAGNOSIS
Multiple theories attempt to explain why Black individuals and other ethnic minority groups are diagnosed with schizophrenia at disproportionate rates in White-majority societies. These include sociopolitical, medical, and biological perspectives.
THEORY 1: SOCIAL DISADVANTAGE AND RACIAL PREJUDICE
One explanation is that Black individuals in White-majority societies experience greater socioeconomic and racial inequalities, which may lead to higher rates of schizophrenia diagnoses. Studies suggest that factors such as police racial profiling, school exclusions, poorer job opportunities, and exposure to racial violence (Harralambous) contribute to higher levels of psychological distress, potentially leading to increased psychiatric referrals and diagnoses.
A counter-argument is that other marginalised ethnic groups, such as East Asians, do not exhibit similarly high schizophrenia rates. However, it has been argued that East Asian communities may underreport mental health issues due to cultural stigma, meaning their true incidence of schizophrenia may be underestimated.
THEORY 2: CLINICAL MISDIAGNOSIS DUE TO CULTURAL DIFFERENCES
Another theory suggests that psychiatrists misinterpret culturally specific behaviours as psychotic symptoms. Some examples include:
Spiritual beliefs in Caribbean and African communities (e.g., talking to deceased relatives) may be seen as hallucinations rather than everyday cultural practices.
Expressive emotional distress in Caribbean cultures may be mistaken for psychotic agitation rather than grief.
Lack of familiarity with African or Caribbean dialects and mannerisms may create communication barriers, making it more difficult for clinicians to accurately assess symptoms.
A critique of this theory is that many Black individuals in the UK and the US are fully assimilated into Western culture, so cultural misunderstandings should not explain all cases of overdiagnosis. Furthermore, Black communities are diverse, with people originating from different continents, countries, and cultural backgrounds—making the idea of a single “Black culture” oversimplified.
THEORY 3: VITAMIN D DEFICIENCY IN BLACK MOTHERS DURING WINTER MONTHS
A biological explanation proposes that Black mothers who are six months pregnant during winter in Northern Hemisphere countries are at higher risk of giving birth to children who develop schizophrenia due to vitamin D deficiency.
Vitamin D is essential for foetal brain development, particularly around the sixth month of pregnancy, when significant cortical development occurs.
Black individuals have evolved to synthesise vitamin D more slowly, originating from sun-rich equatorial regions.
In Northern Hemisphere countries, Black individuals experience less sunlight exposure, potentially leading to vitamin D deficiency during pregnancy.
Studies suggest that children born to Black mothers who were six months pregnant during winter may be more likely to develop schizophrenia later in life.
Supporting evidence comes from research on El Niño weather patterns, which shows that reduced sunlight exposure has been correlated with peaks in schizophrenia diagnoses 15 years later.
A counterpoint to this theory is that South Asian populations also have high melanin levels but do not exhibit the same disproportionately high schizophrenia rates. Possible explanations include:
Dietary Habits – Traditional South Asian diets include foods rich in vitamin D, such as fatty fish and fortified dairy products, which help compensate for lower sun exposure.
Cultural Practices—Certain South Asian communities have greater exposure to outdoor sunlight, particularly in early childhood, thereby reducing vitamin D deficiency.
Genetic Factors – South Asian populations may have different genetic adaptations for vitamin D metabolism, mitigating the risks associated with deficiency.
Additionally, a Danish study analysing neonatal blood samples found that individuals with vitamin D deficiency at birth had a 44% increased risk of developing schizophrenia in adulthood (QBI, 2018). Further research also suggests that vitamin D supplementation in early childhood is linked to lower schizophrenia rates (PMC, 2012).
CONCLUSION
Cultural differences significantly impact the reliability of schizophrenia diagnosis, with Black individuals more likely to be diagnosed with schizophrenia in Western societies. This discrepancy is multifaceted, involving sociopolitical factors, clinical misdiagnosis, systemic biases, and biological influences. Addressing cultural biases in psychiatric training, improving diagnostic criteria, and promoting research into biological risk factors are essential to ensure more accurate and equitable mental health care across diverse populations.
ASSESSMENT
What terms are used by psychologists to describe A and B below? (Total two marks)
A When a person has two or more disorders at the same time.
B When two different disorders have a symptom in common.What terms are used by psychologists to describe A and B below? (Total two marks)
A When a person has two or more disorders at the same time.
B When two different disorders have a symptom in common.
In the context of schizophrenia, outline what is meant by co-morbidity. (Total two marks)
Explain how symptom overlap might lead to problems with the diagnosis and/or classification of schizophrenia. (Total two marks)
Briefly outline and evaluate one study on the validity of the diagnosis of schizophrenia. (four marks)
MATCHING DESCRIPTIONS TO TERMS: For each description, choose a term that best represents that description.
Write the correct letter alongside the relevant term in your answer for each description. (Total four marks)DESCRIPTIONS
A – When a diagnosis is consistent between psychiatrists
B – When a person has more than one condition at the same time
C – When a psychiatrist diagnoses a condition correctly
D – When two conditions have some effects in commonOutline what is meant by reliability in the diagnosis of schizophrenia. (2)
Outline what is meant by validity in the classification of schizophrenia. (2)
Define co-morbidity in relation to schizophrenia. (2)
What is meant by symptom overlap? (2)
Identify one problem with diagnosing schizophrenia. (1)
Outline two problems associated with the classification of schizophrenia. (6)
Outline one issue of reliability in diagnosing schizophrenia. (4)
Outline how cultural bias may affect the diagnosis of schizophrenia. (4)
Outline what psychologists mean by gender bias in schizophrenia diagnosis. (4)
Outline the Reliability and Validity in the Diagnosis and Classification of Schizophrenia (6).
A psychiatrist diagnoses Malik with schizophrenia after a short interview. A later psychiatrist disagrees and gives a different diagnosis. Explain what this example suggests about reliability in schizophrenia diagnosis. (4)
Maria reports hearing the voice of a deceased relative, which is normal in her culture. A clinician diagnoses schizophrenia. Using your knowledge of cultural bias, explain one problem with this diagnosis. (4)
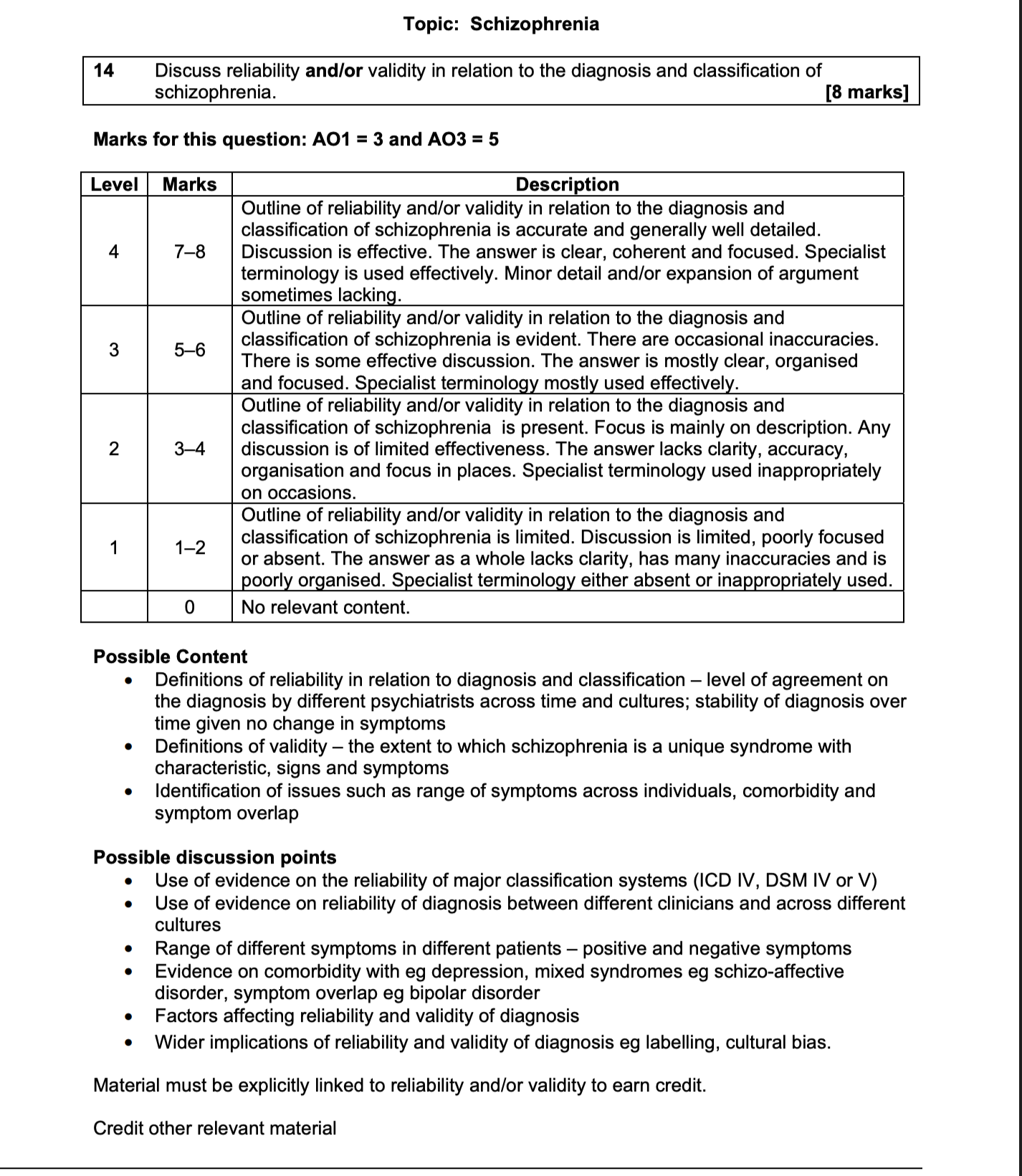
Discuss the reliability and/or validity of the diagnosis and classification of schizophrenia. (Total eight marks)
‘In an important and influential criticism of the diagnosis of mental illness, Rosenhan (1973) showed that healthy ‘pseudopatients’ could gain admission to a psychiatric hospital by pretending to have auditory hallucinations. Although systems of classification and diagnosis have changed considerably since the 1970s, many people still have concerns about their accuracy and appropriateness.’ Discuss issues surrounding the classification and diagnosis of schizophrenia. (Total 16 marks)
Discuss issues associated with the classification and/or diagnosis of schizophrenia. (Total 16 marks).
MARK SCHEME FOR A 16-MARKER
Advice from the AQA mark scheme on this question
Outline and evaluate issues surrounding the classification and diagnosis of Schizophrenia concerning reliability and validity.
AO1 = six marks
AO1 credit is awarded for describing issues concerning the classification and diagnosis of schizophrenia, most of which are related in some way to reliability and validity. Some issues are specifically relevant to schizophrenia, e.g., the range of symptoms / sub-types of schizophrenia and the difficulty of distinguishing between them. Other issues surrounding the classification and diagnosis of mental disorders, in general, can receive credit if they are made relevant to schizophrenia.
For AO1 credit candidates, they need to identify some of these issues. For example:
1) The reliability of the major classification systems (ICD and DSM)
2) The lack of homogeneity (consistency) in schizophrenic symptoms
3) The problem of co-morbidity with depression4) The availability of other diagnostic criteria for schizophrenia, e.g. Schneider criteria
5) Cultural differences in symptom presentation
6) The lack of objective tests for schizophrenia
7) The difficulty of being able to predict outcome or response to treatment
8) The question of whether schizophrenia is a mental disorder at all or a form of political control (Szasz)
Examiners should be mindful of a depth/breadth trade-off – candidates can describe a few issues in detail or more issues in less detail. There is considerable overlap between the problems of classification and diagnosis, so partial performance criteria do not apply. Candidates who offer lists of signs and symptoms of schizophrenia or who describe classification systems are not addressing the issues surrounding diagnosis and classification. Such material is rudimentary.
AO2/AO3 = 10 marks
Candidates achieve AO3 credit by evaluating and offering commentary on the issues they have identified, for example, considering the consequences of the issue. They may discuss the advantages of using classification systems for effective treatment programmes and support and problems associated with classification and diagnosis. For example, the diagnosis might lead to labelling and stigmatisation (Scheff 1966), causing long-term problems in getting/keeping employment and leading to a self-fulfilling prophecy.
EXAMINER’S COMMENTS
Schizophrenia remains the most popular option, and this question was attempted by over half of students. Some schools and colleges had prepared their students for a question on issues regarding The Reliability and Validity in the Diagnosis and Classification of Schizophrenia. Including Reference to Co-Morbidity, Culture and Gender bias, and Symptom overlap, others appeared to have covered this in insufficient depth. AO1 credit was awarded for the identification/description of matters relating to classification and diagnosis, most of which can be placed under the headings of reliability and validity. Weaker answers often showed little evidence of organisation or planning, with students producing long lists of clinical characteristics without identifying issues relating to classification or diagnosis. This approach gained rudimentary AO1 credit.
A lack of focus on the question was also notable for AO2 / 3 with weaker students. Many focussed almost exclusively on Rosenhan’s 1973 study, ‘On being sane in insane places,’ often providing lengthy and detailed descriptions without linking this to an issue related to classification or diagnosis. Weaker students also focused on the methodological evaluation of this research study, which was of limited relevance to the question. There was little recognition that Rosenhan’s study is over 40 years old and has changed classification and diagnosis since then.
Stronger students approached the question by identifying an issue (such as the lack of reliability between ICD and DSM IV) and then considering possible consequences of this and/or research evidence regarding the reliability of diagnosis using the respective systems. There was some helpful discussion of the problems of co-morbidity, cultural differences and Szasz’s critique of the myth of mental illness in better answers. Higher AO2 / 3 marks went to students who evaluated each issue as they went through the essay. Those students who could consider various research evidence relating to reliability and validity were also rewarded.
ESSAY EXEMPLAR FOR RELIABILITY AND VALIDITY IN THE CLASSIFICATION AND DIAGNOSIS OF SCHIZOPHRENIA
VALIDITY
HOW STUDENTS SHOULD WRITE THE VALIDITY SECTION
AO1
Define validity.
Explain why validity matters in psychiatric diagnosis.
Explain that validity concerns whether schizophrenia represents a genuine and distinct disorder with consistent symptoms, causes, biological mechanisms, and treatment responses.
Explain that if the construct lacks validity, research findings into aetiology, brain abnormalities, genetics, and drug treatments will be inconsistent because different underlying conditions may be grouped under the same label.
Explain the knock-on consequences: unclear causes, contradictory biological findings, and inconsistent treatment outcomes.
AO3
Then introduce the factors that challenge validity:
The heterogeneity of schizophrenia symptoms, particularly the distinction between positive and negative symptoms.
Differences in neurobiology, including variation in dopamine receptor activity and different brain regions associated with different symptom clusters.
Variation in treatment response, where antipsychotics tend to reduce positive symptoms more effectively than negative symptoms.
Differences in course and development, with some patients showing chronic deterioration while others show episodic patterns.
Changes in diagnostic definitions across DSM and ICD editions, including the removal of schizophrenia subtypes.
Continuing disagreement between DSM and ICD criteria.
The breadth of the diagnosis, where individuals may share very few symptoms despite receiving the same label.
Unclear boundaries with other disorders, for example, antipsychotics being used to treat mania in bipolar disorder, while highly dissimilar symptoms remain grouped together under schizophrenia.
These points demonstrate that schizophrenia may represent a heterogeneous cluster of conditions rather than a single, clearly defined disorder
AO1: WHAT VALIDITY MEANS AND WHY IT MATTERS
Validity refers to whether a diagnostic category represents a genuine and distinct disorder. In other words, the diagnosis should correspond to a real condition with a coherent pattern of symptoms, underlying biological mechanisms, predictable development, and consistent treatment response.
Validity is important because diagnosis forms the foundation of psychiatric research and treatment. If the construct of schizophrenia is not valid, then research into its causes, biological basis, and treatment will produce inconsistent findings. This lack of validity can appear indirectly through problems such as inconsistent research results, unclear aetiology, or unreliable treatment outcomes. Weak validity, therefore, produces knock-on problems across the entire field, including difficulties in identifying biological causes and inconsistent responses to antipsychotic medication.
EVALUATION VALIDITY
AO3: EVIDENCE THAT CHALLENGES VALIDITY
One major challenge to validity is the heterogeneity of schizophrenia symptoms. The diagnosis includes both positive symptoms, such as hallucinations and delusions, and negative symptoms, such as avolition, flat affect, and social withdrawal. These symptom groups differ substantially in their biological basis, neurological location, and treatment response.
For example, positive symptoms are often associated with increased dopamine activity in subcortical pathways involving D2 receptors, whereas negative symptoms are more commonly linked with reduced dopamine activity in the prefrontal cortex. This suggests that different neurobiological mechanisms may be involved within what is currently treated as a single disorder.
Variation also appears in treatment response and outcome. Some patients respond well to dopamine-blocking antipsychotic drugs, particularly for positive symptoms, while negative symptoms are often resistant to treatment. If individuals with the same diagnosis respond very differently to treatment, this suggests underlying heterogeneity within the disorder.
Another issue concerns differences in course and development. Some individuals experience a chronic deteriorating condition, whereas others show episodic symptoms with periods of recovery. This variation in progression raises further questions about whether schizophrenia represents a single illness.
Diagnostic criteria themselves have also changed repeatedly. Successive editions of DSM and ICD have revised symptom thresholds and removed previous subtypes such as paranoid and catatonic schizophrenia. These changes partly reflect improved research tools and greater knowledge, but they also demonstrate that the disorder's boundaries are unstable.
Even today, DSM and ICD criteria do not fully agree, meaning that the same individual may receive different diagnoses depending on which system is used.
A further conceptual problem is the diagnostic category's breadth. Diagnostic systems allow many different symptom combinations, meaning that two individuals diagnosed with schizophrenia may share very few symptoms. DSM criteria even allow considerable variation in presentation, making the category difficult to falsify.
Finally, diagnostic boundaries with other disorders remain unclear. Antipsychotic medication is also used to treat conditions such as mania in bipolar disorder, yet classification systems maintain these as separate disorders while simultaneously grouping together highly dissimilar positive and negative symptoms within schizophrenia itself. This inconsistency further challenges the construct's validity.
A final point is that problems with validity often become visible through other weaknesses in the system. For example, inconsistent findings in biological research, difficulties in identifying clear causes, and disagreements among clinicians about diagnosis may all indicate that the underlying construct itself is too broad or poorly defined. In this way, weak validity can manifest indirectly through problems such as unreliable diagnosis, inconsistent treatment outcomes, and unclear aetiology.
RELIABILITY
HOW STUDENTS SHOULD WRITE THIS SECTION
AO1
Define reliability.
Explain why it matters.
Explain that poor reliability suggests schizophrenia may be badly operationalised.
Explain the knock-on effects for research samples, diagnosis, and treatment.
AO3
Then bring in evidence:
doctors disagree, DSM and ICD disagree, cultures interpret symptoms differently, gender and ethnicity affect diagnosis, and research studies demonstrate these patterns.
HOW STUDENTS SHOULD WRITE THE RELIABILITY SECTION
AO1
DEFINE RELIABILITY
Reliability refers to the consistency of diagnosis. If a schizophrenia diagnosis is reliable, different clinicians assessing the same individual should reach the same conclusion.
EXPLAIN THAT RELIABILITY CONCERNS AGREEMENT BETWEEN DIAGNOSIS
Reliability focuses on whether clinicians apply diagnostic criteria consistently. The issue is not whether schizophrenia exists as a disorder but whether psychiatrists consistently identify the same symptoms and apply the criteria similarly.
EXPLAIN WHY RELIABILITY MATTERS
Diagnosis must be consistent so that clinicians, hospitals, and researchers are referring to the same condition. If reliability is poor, diagnosis becomes dependent on the individual clinician rather than the patient’s symptoms.
EXPLAIN THAT POOR RELIABILITY INDICATES PROBLEMS WITH THE APPLICATION OF DIAGNOSTIC CRITERIA
If clinicians interpret hallucinations, delusions, or disorganised thinking differently, the same individual may be diagnosed differently. This suggests the diagnostic criteria may not be operationalised clearly enough.
EXPLAIN THE CONSEQUENCES OF POOR RELIABILITY
This has important consequences. If reliability is weak, research samples may be contaminated because studies do not investigate the same disorder across participants. That in turn affects findings on aetiology, brain abnormalities, genetics, prognosis, and treatment effectiveness. Clinically, poor reliability can lead to inappropriate diagnosis and, therefore, inappropriate treatment, since the person may be medicated or managed on the basis of an inconsistent label.
So the AO1 point is not just that reliability means consistency. It is that poor reliability reveals a weakness in the definition and application of schizophrenia as a diagnostic category, and this has knock-on effects for research and treatment.
EVALUATION A03
These findings demonstrate that diagnosis can vary depending on clinician judgment, cultural context, and classification systems, indicating limitations in the reliability of schizophrenia diagnosis.
Evidence for poor reliability comes from differences between clinicians, cultures, genders, and classification systems.
One problem is inter-rater reliability. Different psychiatrists may interpret the same symptoms differently, especially when diagnosis depends on subjective judgements about delusions, hallucinations, disorganised speech, or bizarre behaviour. This means two clinicians can assess the same patient and reach different conclusions.
A second problem is disagreement between classification manuals. DSM and ICD have not always used identical criteria. You can use old studies, like “Being insane in Insane places,” but it is fifty years old. DSM has changed, so has ICD. Bottom line, though, evidence still shows that inter-rater reliability can still be very poor. And there are still differences between DSM-5 TR and ICD-11.
A second problem is disagreement between classification manuals. DSM and ICD have not always used identical criteria, and even modern editions do not fully align. This means the same person may be diagnosed under one system but not another. That immediately weakens reliability because diagnosis depends partly on which manual is used rather than on the patient’s condition alone. Even modern editions do not fully align. This means the same person may be diagnosed under one system but not another. That immediately weakens reliability because diagnosis depends partly on which manual is used rather than on the patient’s condition alone.
A third issue is cultural variation. Behaviour considered psychotic in one culture may be interpreted differently in another. Beliefs or experiences that appear bizarre from a Western psychiatric perspective may be normal within a particular religious or cultural setting. This makes diagnosis less consistent across countries and ethnic groups, and suggests that reliability is partly shaped by cultural assumptions rather than purely by symptoms.
A fourth issue is gender bias. Men are more often diagnosed with schizophrenia than women, but this may partly reflect differences in interpretation. Women may present with more affective symptoms and therefore be diagnosed with mood disorders instead, whereas men may be more readily classified as schizophrenic. If diagnosis changes according to gendered expectations, reliability is weakened.
Research evidence supports these concerns. Cheniaux et al. found that when psychiatrists used DSM and ICD criteria on the same patients, different numbers were diagnosed with schizophrenia depending on the system used. This directly shows poor reliability across classification manuals.
Evidence also comes from studies of clinician and cultural bias. Copeland et al. gave psychiatrists from the US and the UK the same case descriptions and found American psychiatrists were more likely to diagnose schizophrenia than British psychiatrists. Because the patients were identical on paper, the difference must have come from diagnostic practice rather than the individuals themselves. This shows that reliability is reduced across national and professional contexts.
Support for gender and cultural bias also comes from Loring and Powell, who found that psychiatrists were more likely to diagnose schizophrenia in black patients than white patients when presented with otherwise similar case material. This suggests that diagnosis is not applied consistently and may be influenced by stereotypes as well as symptoms.
However, reliability has improved over time because modern manuals use more explicit symptom criteria and structured interviews. That means diagnosis is less impressionistic than it once was. Even so, because schizophrenia still involves subjective interpretation and broad symptom combinations, reliability remains a significant issue.